TIBSOVO FILM-COATED TABLET 250MG [SIN17485P]
Active ingredients: TIBSOVO FILM-COATED TABLET 250MG
Last updated 21 July 2026
Product Info
TIBSOVO FILM-COATED TABLET 250MG
[SIN17485P]
Product information
Active Ingredient and Strength | IVOSIDENIB - 250 MG |
Dosage Form | TABLET, FILM COATED |
Manufacturer and Country | HOVIONE FARMACIÊNCIA, S.A. - PORTUGAL |
Registration Number | SIN17485P |
Licence Holder | SERVIER (S) PTE LTD |
Forensic Classification | PRESCRIPTION ONLY MEDICINES |
Anatomical Therapeutic Chemical (ATC) code | L01XM02 |
Prescription-only Medicines with Exemptions for Supply without Prescription | NA |
Indication
4.1 Therapeutic indications
Tibsovo in combination with azacitidine is indicated for the treatment of adult patients with newly diagnosed acute myeloid leukaemia (AML) with an isocitrate dehydrogenase-1 (IDH1) R132 mutation who are not eligible to receive standard induction chemotherapy (see section 5.1 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Tibsovo monotherapy is indicated for the treatment of adult patients with locally advanced or metastatic cholangiocarcinoma with an IDH1 R132 mutation who were previously treated by at least one prior line of systemic therapy (see section 5.1 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Dosing
4.2 Posology and method of administration
Treatment should be initiated under the supervision of physicians experienced in the use of anti-cancer medicinal products.
Before taking Tibsovo, patients must have confirmation of an IDH1 R132 mutation using an appropriate diagnostic test.
Posology
Acute myeloid leukaemia
The recommended dose is 500 mg ivosidenib (2 x 250 mg tablets) taken orally once daily. Ivosidenib should be started on Cycle 1 Day 1 in combination with azacitidine at 75 mg/m2 of body surface area, intravenously or subcutaneously, once daily on Days 1–7 of each 28-day cycle. The first treatment cycle of azacitidine should be given at 100% of the dose. It is recommended that patients be treated for a minimum of 6 cycles.
For the posology and method of administration of azacitidine, please refer to the full product information for azacitidine.
Treatment should be continued until disease progression or until treatment is no longer tolerated by the patient.
Cholangiocarcinoma
The recommended dose is 500 mg ivosidenib (2 x 250 mg tablets) taken orally once daily.
Treatment should be continued until disease progression or until treatment is no longer tolerated by the patient.
Missed or delayed doses
If a dose is missed or not taken at the usual time, the tablets should be taken as soon as possible within 12 hours after the missed dose. Two doses should not be taken within 12 hours. The tablets should be taken as usual the following day.
If a dose is vomited, replacement tablets should not be taken. The tablets should be taken as usual the following day.
Precautions to be taken prior to administration and monitoring
An electrocardiogram (ECG) must be performed prior to treatment initiation. Heart rate corrected QT (QTc) should be less than 450 msec prior to treatment initiation and, in the presence of an abnormal QT, practitioners should thoroughly reassess the benefit/risk of initiating ivosidenib. In case QTc interval prolongation is between 480 msec and 500 msec, initiation of treatment with ivosidenib should remain exceptional and be accompanied by close monitoring.
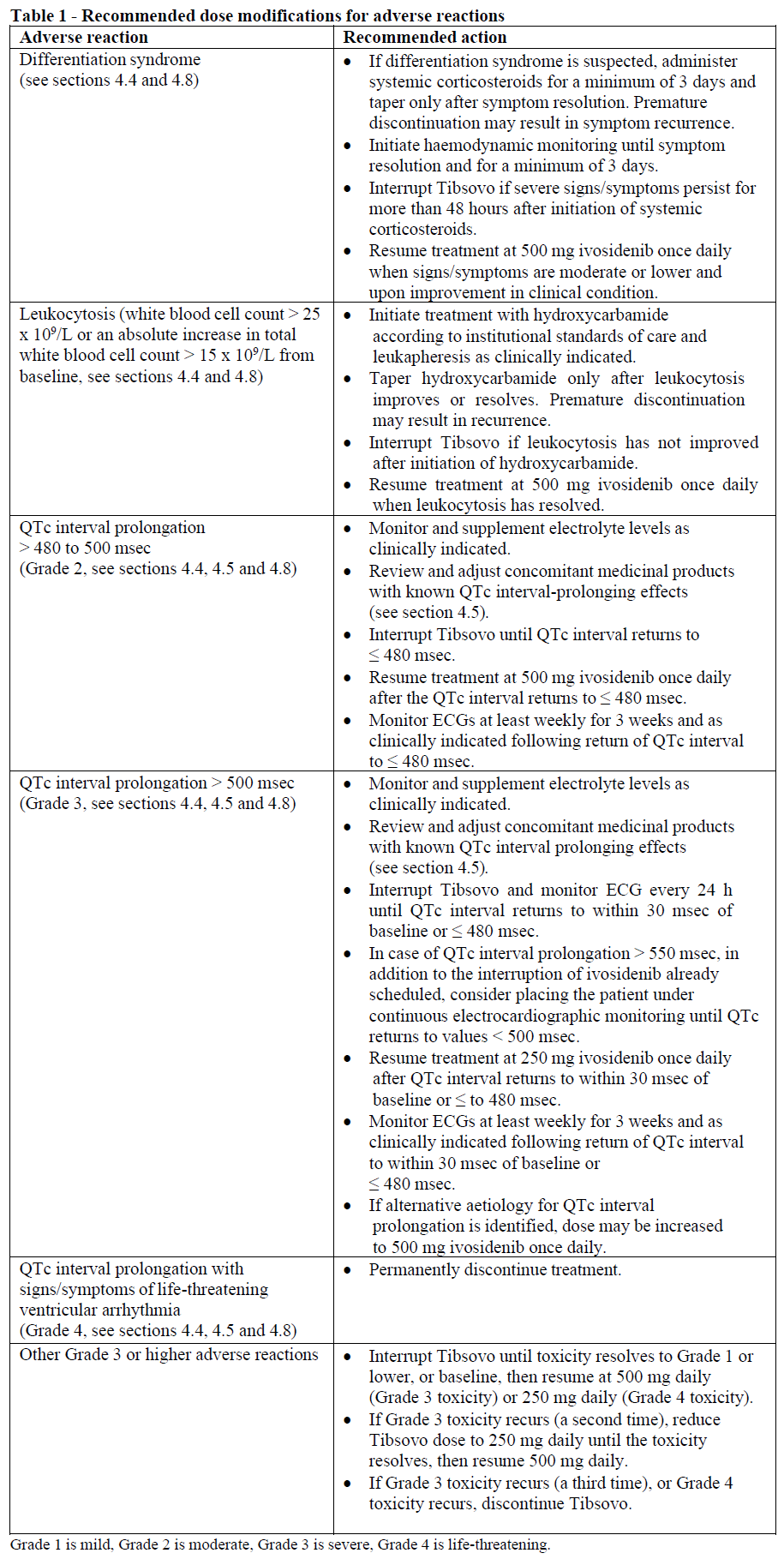
An ECG must be performed prior to treatment initiation, at least weekly during the first 3 weeks of therapy and then monthly thereafter if the QTc interval remains ≤ 480 msec. QTc interval abnormalities should be managed promptly (see Table 1 and section 4.4 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information). In case of suggestive symptomatology, an ECG should be performed as clinically indicated.
Concomitant administration of medicinal products known to prolong the QTc interval, or moderate or strong CYP3A4 inhibitors may increase the risk of QTc interval prolongation and should be avoided whenever possible during treatment with Tibsovo. Patients should be treated with caution and closely monitored for QTc interval prolongation if use of a suitable alternative is not possible. An ECG should be performed prior to co-administration, weekly monitoring for at least 3 weeks and then as clinically indicated (see below and sections 4.4, 4.5 and 4.8 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Complete blood count and blood chemistries should be assessed prior to the initiation of Tibsovo, at least once weekly for the first month of treatment, once every other week for the second month, and at each medical visit for the duration of therapy as clinically indicated.
Dose modification for concomitant administration of moderate or strong CYP3A4 inhibitors
If use of moderate or strong CYP3A4 inhibitors cannot be avoided, the recommended dose of ivosidenib should be reduced to 250 mg (1 x 250 mg tablet) once daily. If the moderate or strong CYP3A4 inhibitor is discontinued, the dose of ivosidenib should be increased to 500 mg after at least 5 half-lives of the CYP3A4 inhibitor (see above and sections 4.4 and 4.5 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Dose modifications and management recommendations for adverse reactions
Special populations
Elderly
No dose adjustment is required in elderly patients (≥ 65 years old, see sections 4.8 and 5.2 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information). No data are available for patients aged 85 years or older.
Renal impairment
No dose adjustment is required in patients with mild (eGFR ≥ 60 to < 90 mL/min/1.73 m2) or moderate (eGFR ≥ 30 to < 60 mL/min/1.73 m2) renal impairment. A recommended dose has not been determined for patients with severe renal impairment (eGFR < 30 mL/min/1.73 m2). Tibsovo should be used with caution in patients with severe renal impairment and this patient population should be closely monitored (see sections 4.4 and 5.2 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Hepatic impairment
No dose adjustment is required in patients with mild hepatic impairment (Child-Pugh class A). A recommended dose has not been determined for patients with moderate and severe hepatic impairment (Child-Pugh classes B and C). Tibsovo should be used with caution in patients with moderate and severe hepatic impairment and this patient population should be closely monitored (see sections 4.4 and 5.2 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Paediatric population
The safety and efficacy of Tibsovo in children and adolescents < 18 years old have not been established. No data are available.
Method of administration
Tibsovo is for oral use.
The tablets are taken once daily at about the same time each day. Patients should not eat anything for 2 hours before and through 1 hour after taking the tablets (see section 5.2 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information). The tablets should be swallowed whole with water.
Patients should be advised to avoid grapefruit and grapefruit juice during treatment (see section 4.5 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information). Patients should also be advised not to swallow the silica gel desiccant found in the tablet bottle (see section 6.5 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Contraindications
4.3 Contraindications
Hypersensitivity to the active substance or to any of the excipients listed in section 6.1 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information.
Concomitant administration of strong CYP3A4 inducers or dabigatran (see section 4.5 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).
Congenital long QT syndrome.
Familial history of sudden death or polymorphic ventricular arrhythmia.
QT/QTc interval > 500 msec, regardless of the correction method (see section 4.2 and 4.4 – please refer to the Product Insert/Patient Information Leaflet published on HSA for the full drug information).